Used worldwide and adapted by the World Health Organization, the Chronic Care Model has guided health systems in transforming care for chronic illnesses since the late 1990s.
Chronic Care Model
Used worldwide and adapted by the World Health Organization, the Chronic Care Model has guided health systems in transforming care for chronic illnesses since the late 1990s. It can be applied to a variety of chronic illnesses, health care settings, and target populations. The bottom line is healthier patients, happier care teams, and cost savings.
A guide to high-quality chronic illness care
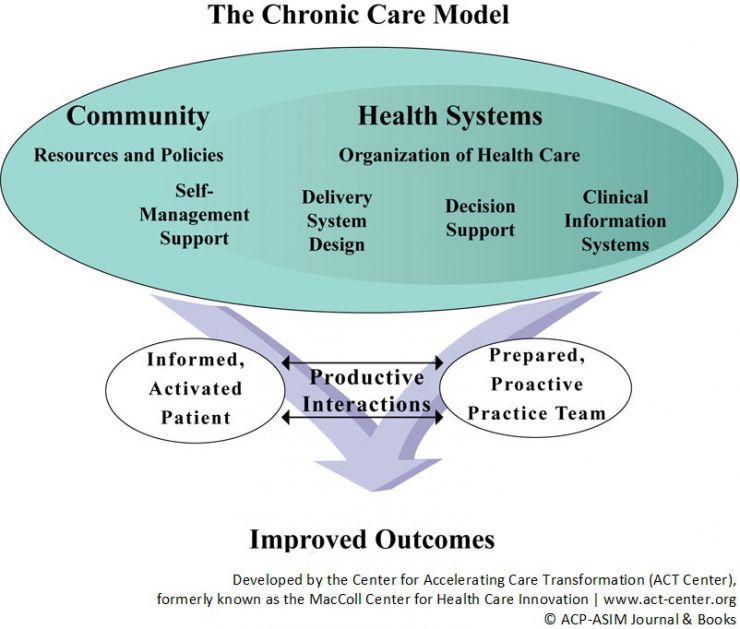
The Chronic Care Model identifies the essential elements of a health care system that encourage high-quality chronic illness care. Within each element of the Chronic Care Model, there are evidence-based principles — or “change concepts” — that teams use to guide their practice transformation efforts. In combination, these change concepts foster productive interactions between people who are well-informed about their chronic conditions and providers who are well-prepared to provide proactive chronic illness care.
Change concepts for the Chronic Care Model
Health System: Create an organization that provides safe, high-quality care
A health system’s business plan reflects its commitment to apply the Chronic Care Model across the organization. Clinician leaders are visible, dedicated members of the team.
Visibly support improvement at all levels of the organization, beginning with the senior leader
Promote effective improvement strategies aimed at comprehensive system change
Encourage open and systematic handling of errors and quality problems to improve care
Provide incentives based on quality of care
Develop agreements that facilitate care coordination within and across organizations
The Community: Mobilize community resources to meet needs of patients
Community resources, from school to government, non-profits and faith-based organization, bolster health systems efforts to keep chronically ill patients supported, involved and active.
Encourage patients to participate in effective community programs
Form partnerships with community organizations to support and develop interventions that fill gaps in needed services
Advocate for policies that improve patient care
Self-Management Support: Empower and prepare patients to manage their health care
Patients are encouraged to set goals, identify barriers and challenges, and monitor their own conditions. A variety of tools and resources provide patients with visual reminders to manage their health.
Emphasize the patient’s central role in managing his or her health
Use effective self-management support strategies that include assessment (physician or self?), goal setting, action planning, problem-solving and follow-up
Organize internal and community resources to provide ongoing self-management support to patients
Delivery System Design: Assure effective, efficient care and self-management support
Regular, proactive planned visits which incorporate patient goals help individuals maintain optimal health and allow health systems to better manage their resources. Visits often employ the skills of several team members.
Define roles and distribute tasks among team members
Use planned interactions to support evidence-based care
Provide clinical case management services for complex patients
Ensure regular follow-up by the care team
Give care that patients understand and that agrees with their cultural background
Decision Support: Promote care consistent with scientific data and patient preferences
Clinicians have convenient access to the latest evidence-based guidelines for care for each chronic condition. Continual educational outreach to clinicians reinforces utilization of these standards.
Embed evidence-based guidelines into daily clinical practice
Share evidence-based guidelines and information with patients to encourage their participation
Use proven provider education methods
Integrate specialist expertise and primary care
Clinical Information Systems: Organize data to facilitate efficient and effective care
Health systems harness technology to provide clinicians with an inclusive list (registry) of patients with a given chronic disease. A registry provides the information necessary to monitor patient health status and reduce complications.
Provide timely reminders for providers and patients
Identify relevant subpopulations for proactive care
Facilitate individual patient care planning
Share information with patients and providers to coordinate care
Monitor performance of practice team and care system
Featured publications on the Chronic Care Model
Katie Coleman, et al. Evidence On The Chronic Care Model In The New Millennium. Health Affairs. Jan-Feb 2009;28(1):75-85
Wagner EH, et al. Organizing care for patients with chronic illness. Milbank Q. 1996;74(4):511-44. doi: 10.1111/1468-0009.12416. Epub 2019 Aug 19.
PROJECT SNAPSHOT
FUNDER
Robert Wood Johnson Foundation
PARTNERS
Institute for Healthcare Advancement
Primary care systems nationwide
KEY CAPABILITIES
Model development
Assessment development
Technical assistance
Dissemination strategy
1999-2010
Re-use of our materials
We encourage the
non-commercial use or adaptation of the materials we develop. With the exception of the Chronic Care Model image, all other materials provided on our site are publicly available, free of cost and copyright protected.